The identity foundation
For the first time, a patient in India can have a single, portable health identity that follows them across hospitals, clinics, labs, and platforms, regardless of which systems those providers use. ABHA (Ayushman Bharat Health Account) makes this possible.
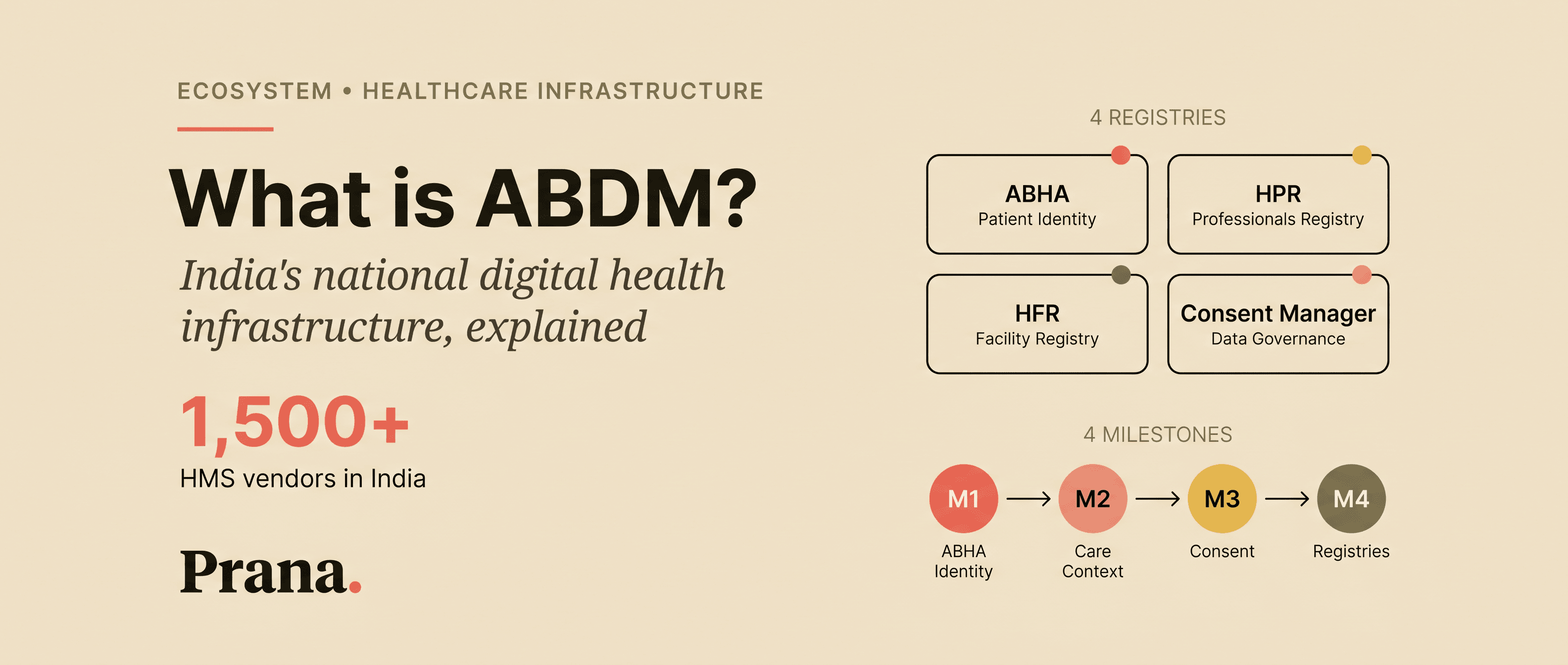
ABHA is not a health app. It is not an electronic health record. It is the identity layer: the foundation that makes everything else in the ABDM ecosystem work.
Two components of ABHA
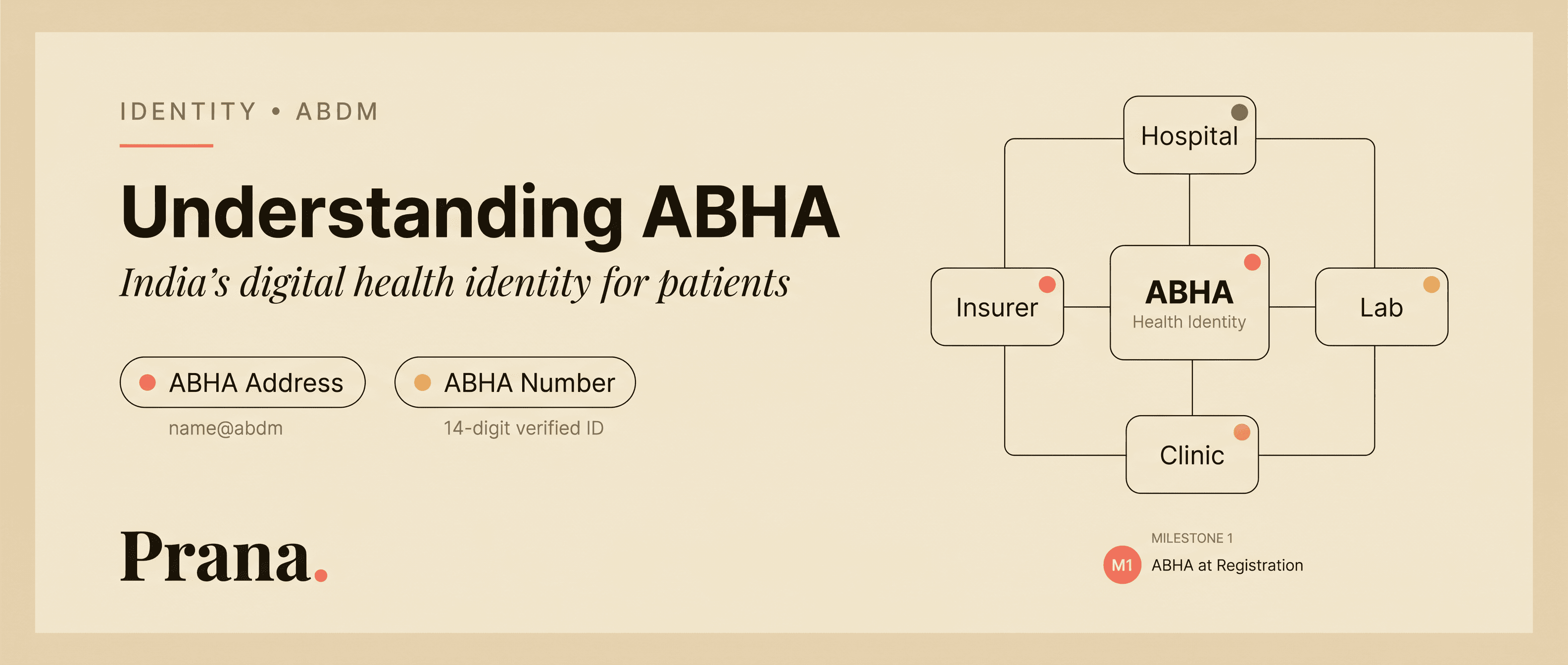
ABHA has two distinct components that serve different purposes:
ABHA Address is a human-readable username in the format name@abdm. Patients use this to access, manage, and share their digital health records across providers and systems. It functions as a healthcare-specific identity handle, similar to how an email address identifies you across communication platforms.
ABHA Number is a unique 14-digit identifier issued after KYC verification via Aadhaar. This is the verified, government-linked component of the health identity. Multiple ABHA Addresses can be linked to a single ABHA Number, providing flexibility while maintaining verification.
How ABHA enables interoperability
Without ABHA, patient records cannot be linked, consented, or shared within the ABDM ecosystem. ABHA is the entry point to everything:
Care contexts are linked to ABHA identities. Consent requests are addressed to ABHA holders. Health records are discoverable through ABHA. Every subsequent milestone of ABDM compliance builds on ABHA being in place.
For hospitals, enabling ABHA at patient registration is Milestone 1: the first step in the ABDM integration journey.
Scan and Share: frictionless registration
One of the most tangible ABHA workflows is Scan and Share. When a patient arrives at a facility, they scan a facility-specific QR code to instantly register, share their ABHA profile with the hospital's system, and optionally receive a queue token.
This eliminates manual patient data entry at registration desks, reduces duplication of records across facilities, and connects the visit directly to the patient's ABHA identity, automatically creating the foundation for care context linking.
Why ABHA matters at scale
The real significance of ABHA is not individual convenience. It is systemic interoperability. When every patient has a verified digital health identity, and every facility links records to that identity, the ecosystem gains something it has never had: a consistent, consent-governed way to connect health data across organizational boundaries.
This is the foundational shift that makes healthcare interoperability possible at a national level.
The identity reconciliation challenge
In practice, linking patients to ABHA is not as simple as creating an account. Many patients already exist in multiple systems under slightly different identities: different spellings of names, different phone numbers, address changes over time.
A patient registered as "Ramesh Kumar" at one hospital may be "R. Kumar" at another and "Ramesh K" at a third. Each facility has created its own internal patient ID. Reconciling these into a single, verified ABHA identity requires matching across inconsistent demographic data. This is a non-trivial infrastructure challenge.
For hospitals with large existing patient databases, the transition is not just about new patients getting ABHA at registration. It involves retrospectively linking existing records (thousands or tens of thousands of patient histories) to ABHA identities. This de-duplication and reconciliation process requires tooling that most facilities do not have.
Multi-provider reality
The real value of ABHA emerges when a patient interacts with multiple providers over time. A patient with a chronic condition may see their general physician monthly, visit a specialist quarterly, get labs done at a diagnostic center, and occasionally visit an emergency department.
Without ABHA, each of these providers maintains a separate, disconnected record. The specialist never sees the GP's prescription history. The emergency physician has no access to the chronic condition management plan. Critical information exists, but in the wrong place at the wrong time.
ABHA creates the connective tissue that allows these records to be linked to a single patient identity and shared (with consent) across providers. This is the continuity of care that fragmented systems cannot provide on their own.